


The right pills
A CHRIS health study spinoff investigates the effectiveness of hypertension medications
Data from the CHRIS population study provides the basis for understanding what makes some people resistant to hypertension therapies. The HyperProfile study research team uses biomarkers to measure the effectiveness of certain drugs on one of the biological processes that regulate blood pressure. The next step will be to cross-reference this data with genetic data.
Mrs. Clara is 82 years old and has been taking blood pressure pills with her latte every morning for the past seven years. To be precise, when she started, there was only one pill, then over time the number went up to three: an ACE inhibitor, a diuretic, and a third tablet that she never remembers the name of. Mrs. Clara is very disciplined and so are her doctors - they “adjust” her medication based on regular checkups. Yet, her blood pressure does not settle down and often her “maximum pressure”, or systolic blood pressure, is around 150 even though she is calm, not drunk coffee and has taken her medications.
Mrs. Clara's is a made-up story, but quite a common one. Often out-of-control blood pressure can indeed be blamed on poor discipline in following therapy and improper lifestyles, but there is also a fair share of people resistant to hypertension treatment.
"Among the people who participated in the first phase of the CHRIS study, 1,814 were already on hypertension therapy. However, in about 50 percent of these cases , participants blood pressure was not under control," explains biologist Luisa Foco, one of the leaders of the HyperProfile study. "In some cases, there is definitely room for improvement in therapy, but in others we can say that there is a real resistance to hypertension treatment”.
Hypertension in numbers
The percentage of CHRIS participants with hypertension is about 24 percent. A large proportion of these participants actually brought their hypertension medications with them to their visit. 1,474 people (about 13 percent, including 60 percent men and 40 percent women) were found to have high blood pressure for the first time during the CHRIS visit and were referred to dedicated services.
One in three people in Italy has from high blood pressure, with a slightly larger proportion of cases in men . "This data is likely to increase in the future due to the aging of the population: in fact, as the years go by, artery walls tend to become stiffer and less elastic, leading to an increase in systolic blood pressure," warns Dr. Stefano Barolo, head of the Hypertension and Cardiovascular Risk Outpatient Service at the Silandro Hospital, a partner in the study.
If hypertension is neglected, as unfortunately often happens - especially in young people, it can lead to serious consequences. The European Society for Hypertension recalls, for example, that it increases the risk of heart attack, ischemic or hemorrhagic stroke, chronic renal failure (with dialysis as an extreme consequence), but also the risk of dementia and cognitive impairment.
There are many drugs for hypertension which are often combined with each other
There are four main categories of drugs that are often combined:
1) ACE inhibitors and sartans, or ACEi and ARB, for short. These are the most common medications which effect one of the processes of pressure regulation which we will explain in more detail below.
2) Beta blockers, BB, for short. These decrease the heart's contraction force as well as the heart rate.
3) Calcium channel blockers – CCB is a medication which determines vasodilation
4) Diuretics.
Currently, one of the most widely used combinations against hypertension consists of: ACE inhibitors or sartans, a diuretic, and a calcium channel blocker.
Among the hypertensive CHRIS participants, about 30 percent are taking ACE inhibitors or sartans and, of these, another 18.5 percent are adding a diuretic. 154 people were prescribed with today’s most widely used combination. "We are talking about people who take at least three pills a day, and yet, despite everything, 87 of them, more than 56 percent, still have high blood pressure," Luisa Foco continues. "These are the cases that interest us most, so that we can shed light on a serious problem that still afflicts too many people."
Biomarkers to find out where the therapy gets jammed
The first step in understanding why drugs fail to keep blood pressure under control is to study what happens at the molecular level in people who do not respond to hypertension therapy.
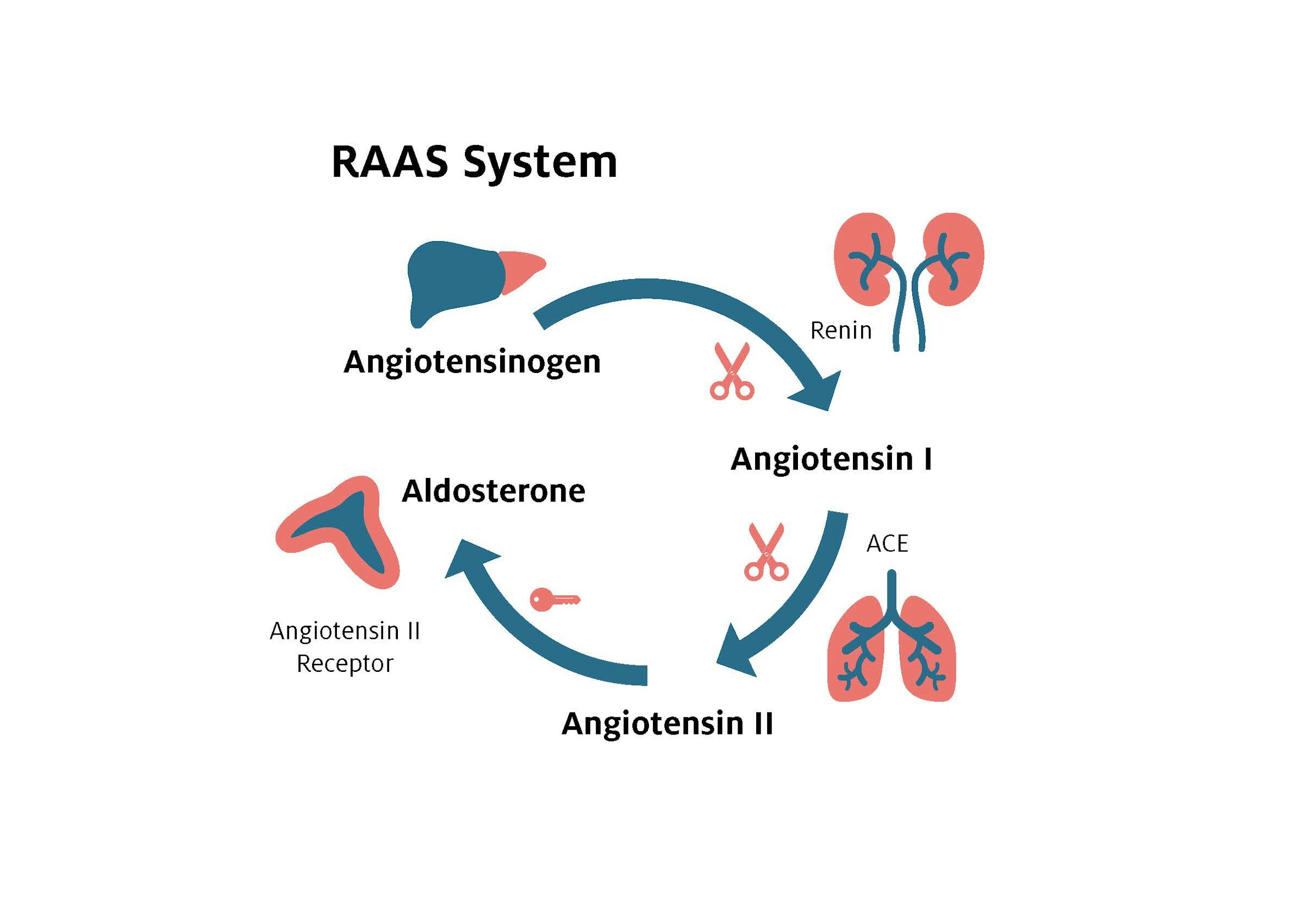
Regulating blood pressure is like a movie in which countless actors play a role, but where the main character is definitely the "renin-angiotensin-aldosterone system" (RAAS for short). This process is the essential long-term regulator of blood pressure.
If pressure gets too low, a protein called renin-because it is secreted by particular renal cells-"cuts" off a fragment from a larger protein produced by the liver: angiotensinogen.
The fragment, called angiotensin I, circulates in the bloodstream and encounters a new protein produced mainly by the lungs, called ACE. Somewhat like renin, ACE also "trims" angiotensin I and converts it into angiotensin II. At this point angiotensin II reaches the adrenal glands and there, binding to its receptor as if it were a key going into the right lock, stimulates the production of aldosterone. This cholesterol-derived hormone prompts our bodies to retain sodium and consequently water and in doing so, eventually raises blood pressure.
In people with hypertension this process is inefficient at various levels.
Most hypertension drugs act to stop this chain. ACE inhibitors which prevent the ACE protein from cutting off angiotensin I and sartans which prevent angiotensin II from binding to its receptor, inhibiting aldosterone production by the adrenal glands as a result are both examples of this.
In the HyperProfile study, Foco and colleagues are looking at six biomarkers for each CHRIS participant that show how this process works. These biological markers show, for example, how active renin and ACE are and, what the function of the adrenal gland is. 800 participant profiles have already been analyzed in detail.
"We have not only had confirmation of when drugs work, but also when they are not effective. For example, you sometimes see people who, while taking sartans, have significantly higher adrenal gland activity than you would expect," Foco explains. "This could mean that their hypertension is a consequence of another disease, primary aldosteronism, and in this case the pressure could be controlled by just changing drugs."
Indeed, the markers studied could direct physicians in choosing the best therapy.
The next step in the study is the genetic analysis, specifically which genes are associated with proteins in the functioning of the renin-angiotensin-aldosterone system?
The HyperProfile study
In addition to Eurac Research's Institute of Biomedicine, research partners include Silandro Hospital, the University of Glasgow and the French research institute Inserm. The study is funded with funds from Law 14 of the Autonomous Province of Bolzano.

